Norah sat down the clipboard. “Stay in your lane,” Dr. Harland Voss said without looking at her, his voice carrying the particular brand of contempt that comes from years of never being questioned. “This is above your pay grade.” She didn’t answer him. She was already at the patient’s side, her fingers finding the pulse before the monitor did, her eyes reading what the machines hadn’t caught yet.
Nobody in that hospital knew where Norah Callahan had been before she walked through their doors 3 years ago. Nobody had asked. And before this night was over, the answer was going to change everything for her, for them, and for the 16 people whose lives hung in the balance between what this hospital thought it was and what it actually needed to be.
If this story already has you on the edge of your seat, follow along, and don’t let go. Hit like, drop a comment with the city you’re watching from, and let’s see how far this story travels. I read every single one. The shift had started badly, which at Callaway Regional meant it had started normally. Norah arrived at 6:47 a.m.
, 13 minutes before she was supposed to, because she always did. The parking lot was still half dark, the kind of February cold that gets into your collar before you’ve even locked the car. And the emergency entrance glowed white and too bright against the pre-dawn sky like something that couldn’t decide if it was welcoming or a warning.
She’d worked enough double shifts to stop noticing the difference. She badged in, grabbed her assignment sheet from the nurses station, and found her name listed under the same ward she’d been assigned to for the past 7 months. General Medical, East Wing, beds 12 through 22. Not trauma, never trauma, despite the fact that she’d put in the transfer request four separate times.
The fourth request had come back with a handwritten note from assistant director of nursing Brenda Pulk that said, “Simply, not at this time.” Norah had folded it in thirds and put it in the same drawer as the other three. You’re on fluids and vitals until 10:00, said Darcy Ren, the charged nurse, finishing the overnight, not looking up from her computer. Darcy wasn’t cruel exactly.
She was the particular kind of tired that comes from working under a bad system for long enough that you stop believing it could be different. Calhoun’s posttop is in 14, needs his dressing changed. 14B is a new admit, chest pain, probably anxiety, but cardiology wants a workup. 12’s been calling the station every 20 minutes about her meal. “Got it,” Norah said.
“Oh, and Voss wants the incident report from Tuesday on his desk by 8.” Norah stopped pulling on her second glove. “The incident report that I already submitted on Tuesday.” He says he didn’t get it. He signed the receipt. Darcy finally looked up. Something passed across her face. Not quite sympathy, not quite guilt, just the exhausted acknowledgement of someone who already knew how this worked.
I know he wants another one. Norah nodded once and went to start her morning. This was the rhythm of her life at Callaway Regional and had been since she joined the staff 34 months ago. She did the work. She did it quietly and without error. She put in requests that were denied, submitted reports that were ignored, made recommendations that were absorbed into the system and credited to someone else or simply discarded.
Last spring, she’d caught a sepsis case that the attendant had missed. A man in his 60s whose presentation was atypical enough that three other nurses had walked past him twice without flagging it. She’d pushed for blood cultures at hour two. The attending, a man named Dr. Price, whose confidence far outpaced his curiosity, had told her to wait for the next vital cycle.
She’d escalated to the charged nurse instead. By hour 4, the cultures had confirmed her suspicion, and the man was in the ICU on the right antibiotics. Doctor Price had presented the case at morning rounds as a complex differential that required careful clinical judgment. Norah had not been mentioned. She knew how to exist inside systems that didn’t see her.
She’d been doing it most of her adult life in one form or another. By 9:15, she’d changed Mr. Calhoun’s dressing, started the cardiology workup on 14B, talked the woman in 12 out of calling the station again by actually sitting with her for 6 minutes and listening, and had drafted the second incident report for Voss. Identical to the first, except she’d CCd the department head this time, small, quiet, documented.
She was reviewing lab results in the hallway when she heard the radio. Not a hospital radio, a scanner, the kind that the security desk kept on low near the side entrance. The feed from Grady County Emergency Dispatch. She’d learned to tune it out months ago, the way you tune out anything ambient when there’s enough other noise.
But something in the cadence of the dispatcher’s voice pulled at her attention in a way she couldn’t immediately name. Multiple vehicle collision. State Route 9 near the Holland Bridge confirmed 15 to 20 civilian casualties, requesting all available units. She went still. First responders on scene reporting at least six critical.
Norah sat down the lab results and walked to the window that faced the parking lot in the road beyond. She could see it from here, the overpass, maybe a mile and a half away, where the red and blue of emergency lights was already blooming against the gray morning like something on fire. She had been in places where that view meant something specific, where the distance between the lights and where you were standing was measured in minutes, not miles, and every one of those minutes cost something.
She turned and walked back to the nurse’s station. Darcy, she said, “The scanner is showing a mass casualty event on Route 9. We need to start activating the surge protocol.” Darcy looked up. Administration gets notified by dispatch. That’s not our call. The protocol says, “Nursing leadership initiates internal prep while admin is being notified, not after.
If we have six or more critical inbounds, we’re going to need the trauma bays cleared, blood bank on standby, and Nora.” Darcy’s voice had that particular flatness. I said, “It’s not our call. Norah looked at her for a moment. Then she turned and walked to the charge phone and dialed the trauma bay supervisor herself.
The supervisor, a laconic man named Gil, who had worked at Callaway for 22 years and had the unhurried certainty of someone who had seen every possible variety of bad day, picked up on the second ring. It’s Nora Callahan from East Medical. I’m looking at the dispatch feed on the scanner. Route 9, Holland Bridge, 15 plus casualties, six critical.
You seeing this? A pause just came through. Voss already knows. I don’t know what Voss knows. I’m calling you. Another pause longer. All right, I’ll start making calls. She hung up. When she turned around, Darcy was watching her with an expression she couldn’t read. Something between irritation and unease. You just went around the chain, Darcy said.
I went to trauma, Norah said. That is the chain. She went back to bed 12. The first ambulance arrived at 9:54 a.m. By 10:20, there were 11 patients in the emergency department, and the waiting room had started filling with people who weren’t from the accident. Regulars, walk-ins, the usual morning crowd who had now been told to wait with no timeline and no explanation, and were handling this with the predictable range of human responses from patient to furious.
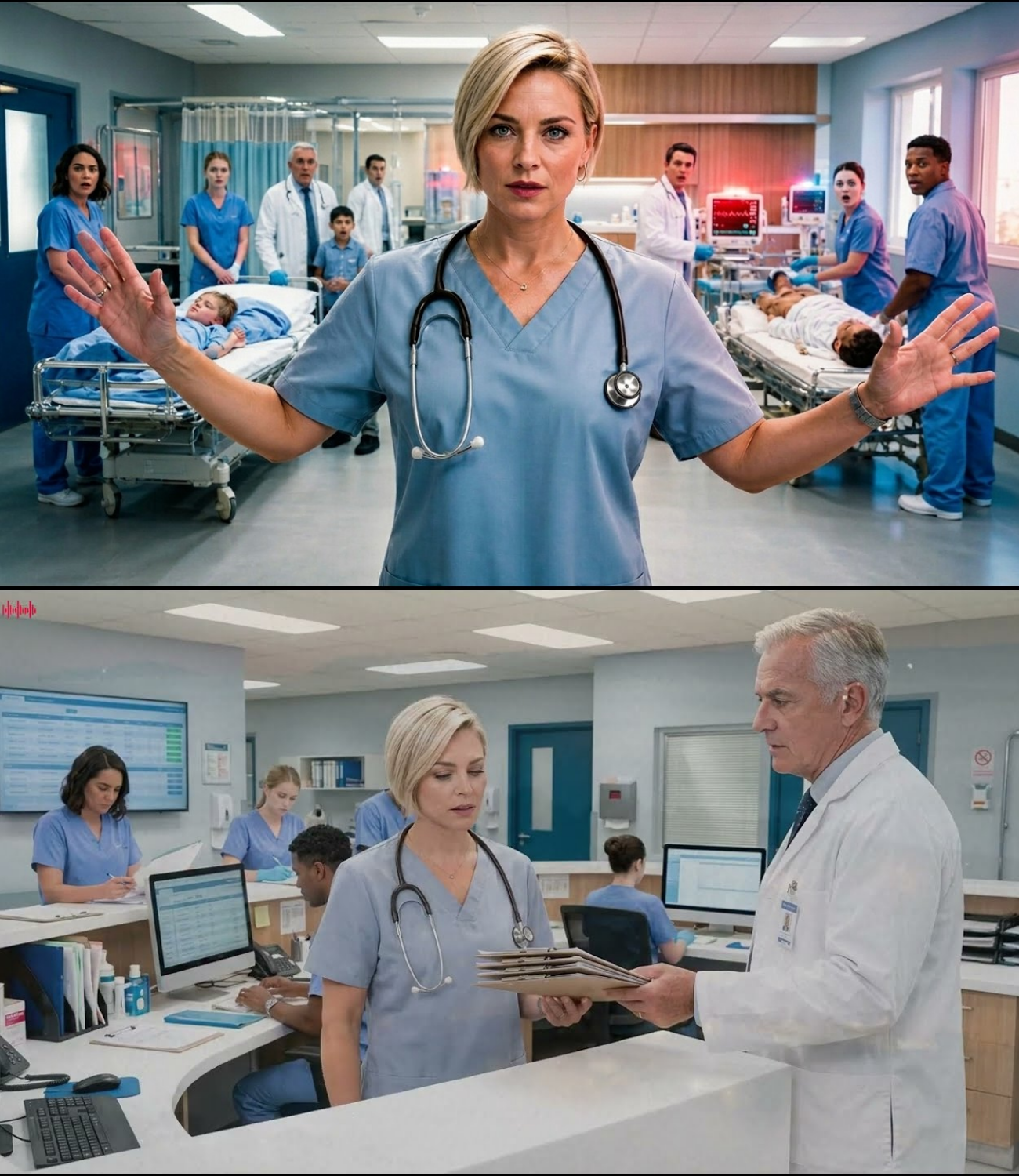
Norah had been pulled to the ED by Gil at 10:08, which was not unusual during a surge. What was unusual was what she found when she got there. The trauma bays were partially cleared but not staged. The blood bank had been called but not yet confirmed. Two of the three attending physicians currently on duty, Dr. Voss and a younger doctor named Reyes, who had been at Callaway for less than a year, were in a heated discussion near the central station about patient sorting while a paramedic stood nearby with a clipboard waiting for someone to give him an answer. The
third attending, doctor Marissa Flint, was the only one actually moving. She was in bay one with a man who’d been extracted from a crushed sedan, and from the sound of things, she was managing without adequate support. Norah took in the room the way she’d trained herself to take in rooms, fast, total, without flinching at any specific thing.
Because flinching cost you the overview. She counted bodies, assessed mobility, clocked the monitors, estimated blood loss on the two patients visible in the open bays, and registered in the background the rhythm of everyone else’s breathing. Who was controlled? Who was running on adrenaline? Who was already starting to fracture? Voss was fracturing.
He was hiding it behind volume and authority, which was a common enough strategy, but she could see it in the way his hands kept moving to his pockets and back out again. She went to the paramedic first. What’s your order of arrival? The paramedic blinked. Uh, the chest trauma in one was first, then we’ve got a 42-year-old with TBI in the hall, three oro casualties in the waiting area, and there’s four more coming in the next unit. ETA 7 minutes.
One of those is pediatric single trauma likely internal mechanism on the pediatric passenger rear impact at speed belt on but the door came in. Norah nodded. Has anyone called pediatric surgery? The paramedic looked at his clipboard. I don’t know. She turned. Reyes. The younger doctor looked over. Culped surgery now.
have them standing by for a possible splenic or hpatic on a minor incoming in seven. Don’t wait for imaging. Reyes opened his mouth, looked at Voss, and hesitated. Dr. Reyes. Her voice didn’t rise, but it had a quality that hadn’t been there before. A precision that didn’t leave room for the hesitation to grow into something. Now he went to the phone.
Voss crossed the floor toward her. He was a tall man, broad in a way that had curdled over the years into something less like strength and more like mass. And he used it the way some people use height as a form of communication. What are you doing? Sorting incoming, she said, already moving toward the TBI patient in the hall.
That’s not your function. You’re a floor nurse, not a trauma nurse, and you were not assigned here by the pediatric case is 7 minutes out and nobody’s called surgery yet, she said, not stopping. We can talk about my assignment after. She heard him say something behind her. She didn’t catch it and didn’t try.
The TBI patient, a woman in her late 50s, conscious but confused, left pupil slightly blown, GCS of 12, and dropping, was on a gurnie in the hallway because all three trauma bays were occupied. A nursing aid was taking her blood pressure with the mechanical cuff. The reading came up just as Norah arrived. 78 over 50, the aid said, his voice tight.
Norah was already at the patients head, pen light in hand. Left pupil sluggish, right reactive. She pressed two fingers under the jaw, corateed pulse weak, but present. She ran her hands along the patient’s scalp with practice speed. Swelling behind the left ear significant. Not from impact, from pressure.
She’s got rising intraanial pressure. Norah said, “I need a physician at this bed right now.” No one came. Voss was back at the station on the phone. Reyes was still on with surgery. Flint was still in bay 1, which was fine. She needed to be. Norah made a decision and went with it. “Get me a BP cuff and keep cycling it every 2 minutes,” she told the aid.
And I need you to go to the station and tell whoever is free that we have a possible epidural hematoma in the hall. Don’t say possible. Say epidural hematoma hall bed needs neurosurgery consult immediately. Those exact words. Okay. The aid said. He was young, 23, maybe 24, and his voice was steadier than his eyes. But he went.
She stayed with the patient and kept talking to her. not clinical reassurance, just talking, grounding, keeping her present in her own body while the pressure inside her skull did what it was going to do. The woman’s name, she’d learned from the intake bracelet, was Dolores Marsh, and she was 57. And the wallet inside her jacket had a photo of what looked like three adult kids and a dog.
Dolores, Norah said, her voice level. I need you to squeeze my hand. A weak squeeze there. Good. You’re doing great. Keep squeezing. The aid came back. Dr. Voss says he’ll assess when he’s call neurosurgery directly. Norah said extension 4417. Tell them epidural hematoma presentation hypotensive GCS12 and falling. They’ll come.
The aid stared at her. Go, she said. He went. By 11:10, the second wave of ambulances had arrived. The pediatric case was in surgery with exactly the right team waiting. Dolores Marsh had been taken for emergency imaging that would confirm what Norah had suspected, and the emergency department had achieved a kind of brutal functional order that it hadn’t had 40 minutes earlier.
It had not been graceful. Two nurses had looked to Nora for direction without anyone telling them to. Gil had started routing incoming to her assessments without comment in the way experienced people sometimes recognize competence without needing to name it. Reyes, to his credit, had stopped hesitating and started moving and was turning out to be a decent clinician when he wasn’t spending energy trying to read Voss.
Voss himself had pulled back into a supervisory posture that could have been described as leadership if you didn’t look too closely. He made announcements. He signed off on things. He had not since her arrival directly interfered with anything she’d done, which was either wisdom or calculation, and she’d stopped trying to distinguish between the two hours ago.
She was at the medication station entering an order when she heard the doors, not the ambulance bay, the main entrance, the heavy automatic doors that opened onto the parking lot. She heard them because of the sound that came through them. Not sirens, not the radio crackle of EMS, something lower and more mechanical, the specific growl of diesel engines that she recognized before she consciously registered why she recognized it.
She looked up through the glass of the entrance in the white gray light of the February morning. She could see vehicles pulling into the lot. Not ambulances, not police cruisers. Three dark green trucks with government plates. Moving with the particular disciplined efficiency that comes from drivers who know exactly where they’re going and have no ambivalence about getting there.
Military vehicles. Her hands went still on the keyboard. One of the vehicles had a communications core insignia on the door. The second had medical cross markings. The third she couldn’t read from this distance, but she didn’t need to. She knew this configuration. She’d seen it deployed on three continents.
Her heart did something complicated and private and she looked back at the monitor and for exactly 4 seconds she allowed herself to feel whatever she was feeling. Then she closed it and went back to work because there were still patients in the hall and a woman named Dolores Marsh who needed someone paying attention.
But her mind was running two tracks now. And she knew with the certainty of someone who has lived long enough inside certain worlds to understand how they operate that the next hour was not going to look like anything she had planned. The doors slid open. A man walked through them in uniform. Army combat uniform, no dress. This was working clothes.
And his rank was visible on his collar before he’d taken three steps inside. Lieutenant Colonel. Behind him, two other service members, one of them carrying what appeared to be a medical deployment bag. The lieutenant colonel’s eyes swept the room with the same rapid intake Norah had performed 40 minutes ago. Same methodology, different training, same instinct. And then his eyes found her.
She didn’t move. He did. He crossed the floor directly toward her. And the way he moved, not rushed, not hesitant, just direct, made two nurses step aside without being asked. He stopped in front of her. He was maybe 40, with a face that had spent time outdoors in unforgiving climates, and his expression as he looked at her was one she couldn’t immediately categorize.
Then he said quietly enough that it was only for her. Sergeant Major Callahan. The room didn’t hear it, but she did. Norah Callahan looked at Lieutenant Colonel James Orard, third special forces group, with whom she had worked in circumstances that neither of them would describe in a hospital corridor, and she said equally quietly. I’m not active anymore.
No, ma’am, he said, but I think you might be running this room. From across the emergency department, Dr. Harlon Voss was watching them. His expression was the particular kind of blank that happens when a person’s mental model of a situation comes apart faster than they can rebuild it. Norah turned back to the monitor.
I’m still in the middle of something, she said to Ord. Give me 4 minutes. Yes, ma’am, he said without irony and waited. It was the ma’am that did it. The reflex of it, the automatic respect encoded into muscle memory that the aid standing 2 ft away heard clearly. that the charge nurse at the station caught that landed in the room like a stone in still water sending out rings that hadn’t finished moving by the time Norah finished entering the order and turned to find out what the army needed behind her.
She didn’t see Voss’s face, but she heard him go very, very quiet. And in the particular acoustics of that emergency department in that hospital in Callaway, Montana on a February morning that had already been the worst day the region had seen in years. His silence was louder than anything he’d said all day. The 4 minutes she’d asked for turned into six because the patient in Bay 3 decided that was the moment to decompensate.
And Norah didn’t leave a decompensating patient for anyone. The man’s name was Curtis Albbright, 44, construction foreman, had been riding in the cab of a work truck when the pileup on the bridge swallowed everything in its path. He’d come in ambulatory, which was the kind of thing that made triage nurses feel cautiously optimistic and experienced trauma clinicians deeply nervous because the patients who walked in sometimes had the worst internal stories.
Norah had flagged him on first look, the way he was holding his side, subtle enough that most people read it as pain management and not as guarding, and had requested an abdominal ultrasound before the initial labs even came back. The ultrasound tech had been pulled to radiology for a stat CT. The labs had been slow, and Curtis Albbright had been sitting in Bay 3 telling everyone he was fine.
He just needed some Tylenol and a phone to call his wife, right up until he wasn’t fine anymore. His pressure dropped first, then the pain broke through the adrenaline that had been masking it, and he went pale in the specific way that happens when the body is redirecting everything it has to the core. And by the time Norah got there, his systolic was in the 80s and falling.
“I need a surgeon in bay 3 now,” she said, loud enough to carry. No one moved immediately, so she put two fingers on Curtis’s wrist and said without raising her voice further. Mr. Albbright, I need you to stay with me. Look at my face. Right here. He looked at her. His eyes were glassy but present. Good, she said.
I’m right here. We’re going to get ahead of this. She had two large bore IVs in his arms before the surgical resident arrived, fluids running wide open. And when the resident, a young woman named Dr. Priya Anand, who moved fast and asked the right questions, came through the curtain, Norah gave her the handoff in 18 seconds flat.
Mechanism, presentation, vital trend, what she’d already done, what she suspected. Anan didn’t waste time. O availability. I can check, Norah said, already reaching for the phone. Please. Anand was at Curtis’s side, hands on his abdomen, her face doing the focused neutral thing that good surgeons learn early. “Sir, I’m Dr. Anand.
I’m going to take care of you.” “My wife,” Curtis said. His voice had gone thin. “We’ll call her,” Norah said. “What’s her name?” “Patricia.” “She she doesn’t know I was on that road.” “We’ll call her,” Norah said again. Right after I make this other call, she got O2 confirmed, got a transport team moving, and was back at the station in under 3 minutes.
Ord was still waiting where she’d left him, standing with the particular stillness of someone accustomed to waiting in worse places than this. His two subordinates had moved to the sidewall and were out of the way of the moving bodies around them in the way of people who understood how to occupy space without consuming it.
Sorry, she said, not because she was apologizing, but because it was accurate. Don’t be, Lord said. I watched. You haven’t changed. I’ve changed plenty. She pulled him toward a quieter section of hallway, a dead-end corridor near the supply closet that gave them maybe 40 ft of space without bodies moving through it.
What are you doing here, James? It wasn’t quite a question. She’d known James Orard for 9 years, and the way he’d come through those doors, the configuration of vehicles, the medical bag, the directness, told her this wasn’t a coincidence, and it wasn’t a routine coordination visit. There were four active duty personnel on that bridge. Hard said three survived.
One of them is critical. We had a medical team doing a training exercise 40 minutes from here. When the call came in, command authorized us to respond and coordinate with the civilian facility. The critical. What’s his status on route? ETA 12 minutes. Blast pattern injury, lower extremities, plus blunt thoracic from the vehicle impact.
He’s got two tourniquets on. Norah’s eyes moved without thinking to the clock on the wall. Who’s your medic? Sergeant Yun. She’s good, but this is He paused, which was not something Or did casually. I wanted you to know we were coming in. I didn’t know you were here until I walked through the door. She believed him.
She also knew that his being here in this hospital, seeing her like this in scrubs with a stethoscope, no rank, no uniform, no context that would explain to anyone watching why a lieutenant colonel had just addressed her with a difference that didn’t compute, was going to require managing, and she was already tired, and the morning was only half done.
“Okay,” she said. Tell Yun to meet me at the ambulance bay in 10 minutes. And James? Yeah. Don’t do anything that makes this harder than it already is. He looked at her for a moment. You mean with the physicians? I mean with any of it. He nodded. He understood. He’d known her long enough to understand what it cost her to exist in a place like this the way she’d been existing.
And he was a smart enough man to know that his showing up with a uniform and a history wasn’t uncomplicated for her. Whatever he was feeling about finding her here, and she could see that there was something tucked behind the professional exterior, he put it away. “10 minutes,” he said. She went back to work. The next 10 minutes were the kind that compressed time strangely, each individual moment crystalline and slow, but the block of them gone before she’d properly registered its passing.
She pulled the trauma bay status, confirmed bay 2 could be prepped for a blast pattern lower extremity presentation, tracked down the vascular surgery attending who was two floors up and needed to be two floors down and found a moment somewhere in the middle of all of it to pick up a phone and call the number that the aid, whose name was Marcus, she’d finally caught it, had found for Patricia Albbright.
The call lasted 45 seconds. Norah told her what she needed to tell her, kept it clear and honest without being brutal, confirmed the hospital address, and hung up before she could get pulled into the emotional weight of it. Not because the emotional weight wasn’t real, because there wasn’t space for it right now, and Patricia Albbright needed a functioning hospital more than she needed a nurse who had let herself drown for a moment in someone else’s fear.
She was halfway to the ambulance bay when Voss appeared in the hallway. He had collected himself. The blank shock she’d seen on his face when Or had crossed the floor toward her was gone, replaced by something harder and more deliberate. He’d had 10 minutes to think, and whatever he’d thought, it had settled into an expression that she’d seen before on other faces in other contexts.
The expression of a person who has decided that the best defense is to establish control before anyone else does. “I need to speak with you,” he said. I have an incoming critical in 8 minutes, she said without stopping. This will take two. Something in his tone made her stop. Not because she was afraid of him, because she’d learned years ago that there were moments when stopping costs less than whatever you left running behind you. She turned.
You’ve been operating outside your scope all morning. He said his voice was low and even, which meant he’d decided that quiet authority was his best instrument. I’ve documented three separate instances where you issued directives to staff and physicians that were not within your authority as a floor nurse.
She looked at him. I understand the situation is unusual, he continued. And I’m not unsympathetic to the instinct to help, but the military’s presence here does not change your employment status or your scope of practice at this facility. I need you to return to a support role for the remainder of this event. She kept looking at him.
He was, she noted, standing slightly sideways to her. Not quite confrontational, not quite differential. The physical grammar of someone who wanted to project authority while leaving himself a retreat if he needed one. Dr. Voss, she said, there’s a soldier with blast injuries coming in in 7 minutes. I have a surgical team standing by.
I have the trauma bay staged. The vascular attending is on his way down. Excellent. then the team is ready and your involvement is no longer necessary. My involvement, she said, is why the team is ready. The air between them had a quality she recognized. She’d been in rooms where that quality existed in more extreme forms, where it was loaded with something other than professional tension, and she’d learned to keep her voice level, and her face readable in those rooms, even when everything underneath was not.
She kept it. Now I’m going to the bay. She said, “If you want to have this conversation, we can have it when the patient is stable.” She walked away. She heard him say behind her, “I’ll be speaking with administration today.” She pushed through the door to the ambulance bay and let it close. Um, Sergeant Firstclass Diego Restrepo was 28 years old and had been in the army for 9 years and he was conscious when they brought him in, which was either a good sign or the worst kind, depending on what was underneath. He was on a backboard with
two cat tourniquets, one on each leg, mid thigh, and the paramedic doing the handoff was talking fast and precise in the way of someone who knew their window was closing. Blast pattern fragmentation. Both lower extremities left worse than right. Right tib fib fracture open. Thoracic contusion. Possible rib fractures.
Breath sounds reduced on the left. Pressure’s been holding at 94 systolic with the tourniquets, but it was 82 when we loaded. GCS15. He’s talking. Restrepo was in fact talking. He was saying something in a voice too low for Norah to catch as she came to his side. And she leaned in. And what he was saying was, “Don’t let them cut my legs off.
Please, please don’t let them.” Nobody’s cutting anything that doesn’t need to go, she said. And she meant it as both fact and promise. The way you sometimes have to mean things simultaneously. I’m Nora. I’ve got you. What’s your pain level? Doesn’t matter. It matters to me. A beat. Seven.
Okay, we’re going to manage that. Sergeant Yun briefed us. You’ve been well taken care of getting here. He looked at her. He had dark eyes and a face that was trying very hard to stay composed and mostly succeeding. You military? Not currently, she said. Something in her voice or her manner or the efficiency of her hands as she checked the tourniquet placement and assessed the left leg’s perusion status or lack of it made him exhale slowly.
Not relaxation, recalibration. The specific adjustment a person makes when they’ve decided to trust the person next to them. The vascular attending doctor Felix Huang arrived 30 seconds later, took one look at the left leg and said to Norah without preamble, “Distlal pulse, absent left, diminished right. How long on the tourniquet?” She looked at the time stamp on the cat.
38 minutes. Wong’s face did the math. We need to move. Can we get him to O sheet? Two is standing by. Norah said. Huang looked at her with the expression of someone reccalibrating their expectations. Not suspiciously. More the way you look at a road that’s better than you expected. Good. Let’s go.
Restrepo grabbed her wrist as the gurnie started moving. My CO, he said. Is he? I don’t have information on the others yet, she said honestly. But we have people working on that. Focus on you right now. He released her wrist. The gurnie moved. Ord was at the edge of the bay. He’d watched the handoff without interfering, which was exactly right.
And when she came back toward him, his expression held something careful. He’s going to surgery, she said. Huang’s good. If the window isn’t already um she stopped. Huang’s good. The other two are stable. Ord said at Mercy General in Dylan. I got the call while you were. He nodded toward the bay. She let out a breath. Not relief exactly, but the release of something she’d been holding without knowing.
Nora or said he wasn’t using her rank now, which was deliberate, and she knew it. I need to tell you something. She waited. The reason I recognized you immediately, it wasn’t just that I know your face. I was briefed before we deployed this morning that there might be a Callaway Regional nurse on scene at the response. Someone from command called ahead.
She went still. Why would command call ahead about me? Because your file came up in a routine review last month. Someone in the Veterans Integration Program ran a cross reference of personnel who’ve transitioned to civilian medical roles. Your name flagged because of your deployment record and your commenation status.
And there was a notation in the civilian personnel system that he paused that you’d been passed over for promotion multiple times despite a performance record that didn’t support the decisions. The hallway around them was still full of movement. Gurnie, staff, the ambient noise of a hospital running at emergency capacity. Norah felt very distinctly as though she were standing slightly outside all of it.
Someone was looking at my file, she said. Someone is looking at a lot of files, ord said carefully. There’s a broader review happening. Civilian medical institutions that have received federal designation and funding in relation to veteran care programs. Callaway Regional is one of 17 hospitals in a three-state region that’s been flagged for how it’s managing or mismanaging personnel with military medical backgrounds.
She was quiet for a moment. She kept her face still. How long has this been going on? She said. It came out flat without inflection, which was what happened when she processed something that was both unexpected and in retrospect entirely logical. The review about 4 months and nobody told me they weren’t supposed to. It’s not He seemed to weigh something.
It’s not an investigation yet. It’s a review. But the people running it are serious. And what I saw this morning in that ED is exactly the kind of thing that’s going to be relevant to what they’re building. Nora looked at the wall. There was a whiteboard on it, the kind hospitals used for patient tracking, full of names and room numbers and status codes and dry erase marker.
Familiar, functional, completely benile. She’d looked at boards like that for 3 years and never once let herself think about the other boards she’d looked at in other rooms where the stakes of the status codes were different in kind, if not in form. James,” she said, “are you telling me this as a professional courtesy, or are you telling me because someone asked you to?” He was quiet for exactly the right length of time.
Long enough to be honest, short enough not to perform it. “Both,” he said. She nodded that she could respect. “All right,” she said. “Then tell whoever’s running the review that they can request my personnel file through the proper channels. I’m not going to perform for an audience. That’s not what I’m That’s I know it’s not what you’re asking me to do.
She turned back toward the ED. I’m still in the middle of a mass casualty event. Are we done? Or looked at her and his face was something that wasn’t quite admiration and wasn’t quite frustration and was probably both in a ratio she didn’t have time to analyze. “We’re done,” he said. She went back in.
By 1:15 in the afternoon, the emergency department had processed 19 patients from the route 9 accident. Three were in surgery. Two were in the ICU. The rest had been stabilized, triaged to appropriate floors, or in the case of four patients with minor injuries, treated and discharged with follow-up instructions.
Dolores Marsh had come back from imaging with a confirmed epidural hematoma and gone directly into neurosurgery. The operating surgeon, a compact woman named Dr. Adas Noachuku, who ran her O like a controlled detonation, had passed Norah in the hallway on her way to scrub in and said without slowing down, “Good catch on the hematoma. Pressure was building fast.
” It was six words and it landed the way competence always lands, clean without ceremony. The pediatric case, a 9-year-old boy named Finn, who had been in the backseat of his mother’s car, had come through splenic repair surgery and was in recovery with his mother in the chair beside him, which was the outcome you fought for and tried not to let yourself feel too much about until it was confirmed because the alternative was you stopped functioning midshift.
Curtis Albbright had been in surgery for 40 minutes. Norah didn’t know his outcome yet and had to set it in the part of her mind where she kept things that weren’t resolved. She was at a workstation entering notes late because everything was late. Her documentation was 3 hours behind when Brenda Palk appeared.
Brenda was the assistant director of nursing, the same woman whose handwritten not at this time notes lived in Norah’s desk drawer. She was in her late 50s, efficient seeming, with the administrative polish of someone who had survived multiple hospital leadership turnovers by being essential to the machinery without being threatening to the people who ran it.
She was not, in Norah’s assessment, a bad person. She was a person who had decided some time ago that managing upward was more important than managing right. Nora, she said, can I have a moment? Norah saved her notes and turned. Of course, Brenda sat down in the chair beside the workstation, which was not something she normally did.
She usually held conversations standing, which kept them brief and vertical, which meant they were on her terms. Sitting meant this was going to be longer, and she knew it. First, Brenda said, “I want to say that what happened today, the response, the patient outcomes is something the hospital can be proud of.” Nora waited. Dr.
Dr. Voss came to me an hour ago, Brenda said. Her voice was even, but Norah had been reading people for long enough to hear what was underneath the evenness. Discomfort, she thought. Not guilt. Brenda wasn’t the guilty type, but genuine discomfort, which was its own thing. He raised some concerns about scope of practice during the event.
I assumed he would. Brenda looked at her. He’s filed a formal report. Okay. Nora. Brenda leaned forward slightly, which meant she was deciding to be direct, which Norah appreciated. “He’s recommending a suspension pending review of your actions this morning.” “Given the nature of the event, the board may want to.” “What was the alternative?” Norah said, not angry, genuinely asking, “The pediatric case would have gone to the O without the right surgical team standing by. Mrs.
Marsh would have been in a hall bed with rising intraanial pressure and nobody moving on it. Sergeant Restrepo would have. I understand. Brenda said, “I do. And I want you to know that I think.” She stopped. Started again. “I think there are things about your background that the hospital hasn’t fully taken into account.” “My background is in my file,” Norah said.
It was the same thing she’d said to herself internally four times over the past 3 years. Out loud, it had a different weight. Brenda went quiet for a moment. Something was working in her face. Some internal calculus, the kind you do when you’ve been operating within a system for long enough that any deviation from it feels structurally risky.
The military personnel, Brenda said finally, “The lieutenant colonel, he knows you. We worked together. He was the way he spoke to you was because of a working relationship that no longer has any bearing on my employment here, nor kept her voice factual, not defensive, factual. If the hospital wants to investigate my actions this morning, I’ll cooperate fully.
I’ll provide documentation of every decision I made and the clinical reasoning behind each one, but I won’t accept a suspension while that review is happening because I haven’t done anything that warrants removing me from patient care. Brenda looked at her for a long moment. “That’s your position,” Brenda said. “That’s my position.” Brenda stood.
She smoothed the front of her jacket, which was a gesture Norah had come to recognize as her way of marking the end of a difficult conversation without resolving it. “I’ll convey that to Dr. Voss and to administration. In the meantime, in the meantime, I have documentation to complete and a patient in surgery I need to follow up on.
” Norah said, “Is there anything else?” There wasn’t. Brenda left. Norah turned back to her workstation and stared at the screen for a moment without typing. The thing that was working in her chest wasn’t anger. She’d moved past anger years ago on this particular subject. Had metabolized it into something quieter and more functional.
What she felt now was closer to a specific weariness. the exhaustion of having to justify again the value of what she’d done in a place that had spent three years deciding her value for reasons that had nothing to do with what she was capable of. She started typing. At 240, Marcus found her. He was still in the slightly stunned state that she’d noticed in him earlier, the look of someone whose mental model of a normal day had been thoroughly dismantled and hadn’t quite reassembled yet.
He was a good aid. She’d clocked that within the first hour of the surge. He asked useful questions. He didn’t freeze under pressure, and he’d followed through on every directive she’d given him this morning without requiring repetition, which was rarer than it should have been. Mrs. Albbright is in the waiting room, he said.
Curtis Albbright’s wife, she the surgery’s done. He’s in recovery, but she asked if she could speak with the nurse who called her. Norah nodded. Give me 5 minutes. She finished the note. she was writing, stood, stretched a back that had been in motion for 7 hours, and went to the family waiting room. Patricia Albbright was 61, compact, with silver streaked hair pulled back in a way that suggested she’d been in the middle of something when she got the call.
She had the particular stillness of someone who has absorbed a large shock and is now running on the focused energy of aftermath. She stood when Norah came in. “You called me,” Patricia said. “I did. I wanted to make sure you heard it clearly and directly. The doctor came out an hour ago. He said the repair went well. She paused.
He also said someone had already ordered the right imaging and had a surgical team ready before Curtis was even critical. The team deserves the credit for the surgery. Norah said. Patricia looked at her with the clear assessing gaze of a woman who had probably spent decades seeing through deflection. That’s not what I asked.
Norah almost smiled. Your husband is going to need some recovery time. The injury was significant, but he’s strong and the surgical repair was clean. Do you have family who can help? Two daughters, Patricia said. They’re on their way. She paused again. He told the paramedic to tell the nurses he was fine. He does that.
He thinks if he says it enough, it becomes true. A lot of people do that. Do you? Norah looked at her. It was an unexpected question, the kind that comes from someone who doesn’t do small talk because they’ve learned it wastes the time you have. Sometimes, Norah said honestly. Patricia nodded as if this confirmed something.
Thank you, she said, for calling me and for whatever you did in there. Norah nodded. She excused herself and went back to the floor. She was at the station pulling Restrepo’s postsurgical status when she heard Voss’s voice from the corridor outside the administrative suite. Loud enough to carry which meant either he was angry enough to have stopped caring about professional register or he wanted to be overheard.
In her experience with men like Voss, it was usually both. Completely outside established protocol and the presence of military personnel does not constitute authorization to she kept her eyes on the screen. cannot have nursing staff making clinical decisions that belong to attending physicians regardless of what her background supposedly.
Supposedly she heard that word and she kept her face neutral and her hands steady and she kept reading Restreo’s chart which showed that he was out of surgery, that Hang successfully restored profusion to both limbs, that both legs were intact and that he was currently in recovery asking for his phone.
She pulled up her email to send a note to the charge nurse about Restrepo’s status. There was a new message in her inbox received 47 minutes ago from an address she didn’t immediately recognize. The subject line read Callaway Regional Personnel Review Inquiry. She opened it. The sender identified themselves as a senior investigator with the Federal Office of Health Systems Oversight.
The message was short, formal, and precise. It stated that as part of an ongoing review of federally designated veteran care facilities, the investigator was requesting Norah’s voluntary participation in a preliminary interview. It listed the review’s scope, personnel practices, promotion decisions, scope of practice determinations, and the phrase that made something cold move through her chest, potential systemic suppression of qualified personnel with military medical backgrounds.
The interview request was dated 3 weeks ago. It had been sitting in a spam folder she hadn’t checked. The message was forwarded. At the bottom below the original inquiry was a single line from a second sender. An internal hospital email address. No name attached. The account was listed under a generic administrative handle.
The line read, “I thought you should have seen this sooner. I’m sorry it took this long.” Norah stared at the screen. Someone inside the hospital had been sitting on this referral for 3 weeks. The question wasn’t whether that had been accidental. The question was who and whether they’d done it on purpose and what they’d been trying to protect.
She looked up from the screen. Across the ED through the glass partition of the administrative suite, she could see Voss talking to Brenda Pulk. He was still talking. His hands were moving with the conviction of a man who believed he was winning something. He didn’t know about the email. She didn’t know yet what the email meant or how far the review had gone, or what the person who’d forwarded it was risking by doing so.
What she knew was that 3 years of being managed, diminished, documented, and quietly buried had just produced a paper trail in both directions, hers and theirs, and that trails in her experience always led somewhere. She picked up her phone and typed a reply to the investigator. I received your message today. I’m available at your convenience.
Please contact me directly at the number below. She attached her personal cell, not the hospital line, hers. She sent it. She set the phone down and for a moment she sat very still in the controlled noise of the emergency department, the monitors, the movement, the low frequency hum of a hospital that had swallowed a disaster and was still functioning.
And she felt the specific clarifying sensation of a situation that had just crossed from one phase into another. From down the corridor, Voss laughed at something. A short satisfied sound on her screen. The scent message confirmation appeared. And from the door of the administrative suite, unhurried with the particular unhurried quality of someone who has just made a decision they’re not going to unmake, Brenda Pulk looked across the department and found Norah’s face and held it for just a second too long before she looked away.
Brenda looked away first. That was the thing Norah kept coming back to. Later, when she was trying to reconstruct the sequence of the afternoon, not Voss’s laugh, not the email, not even the cold particular weight of understanding that someone had sat on a federal inquiry for 3 weeks.
What she kept returning to was the moment Brenda Pulk looked away quickly, precisely, the way you look away from something you’ve already decided not to see. She’d known Brenda for 3 years. In that time, she’d learned to read her the way you learn to read any person whose decisions affect your daily life. The small tells, the specific hesitations, the ways her efficiency occasionally cracked around the edges of something she found uncomfortable.
Brenda was not a villain. Norah had always believed that. But villains were rarely the problem in institutional settings. The problem was the people who knew something was wrong and decided the cost of saying so was higher than the cost of staying quiet. That calculation had just changed. Norah could feel it.
Not in any dramatic sense. No confrontation, no announcement, just the specific atmospheric shift that happens when a situation that has been static for a long time begins to move. She finished her shift notes. She clocked out at 4:18, 17 minutes late, which given the day was almost funny. She drove home in this gray afternoon, made rice and canned soup on her stove because she was too tired to cook and hungry enough that it didn’t matter.
and sat at her kitchen table with her personal laptop open and the federal investigator’s email pulled up on the screen. His name was Arthur Bellamy. She’d looked him up after sending the reply, not because she doubted him, but because she’d spent enough years in environments where verifying was baseline practice.
The Federal Office of Health Systems Oversight was a real entity within the Department of Health and Human Services, its mandate covering exactly what his message described. compliance review of federally funded medical institutions with a specific subdivision created four years ago to address personnel practices affecting veterans and civilian healthcare transition.
Bellamy had been with the office for 11 years. His name appeared on two published review outcomes, both of which had resulted in significant restructuring of hospital administration in other states. This was not a fishing expedition. This was a reel already in the water. She slept 6 hours and was back at the hospital by 7:00 the next morning.
So the building felt different or she felt different inside it. Sometimes those things were the same. She arrived to find her assignment had been quietly changed. No conversation, no written notice, just the sheet at the nurse’s station with her name listed under a different wing. The orthopedic floor on the third level where the morning was reliably slower and the most complex thing she’d manage would be postsurgical vitals and discharge paperwork.
It was, in the language of hospital administration, a repositioning. In any other language, it was a message. She took the assignment sheet, nodded to the charge nurse, who couldn’t quite meet her eyes, and went to the orthopedic floor. By 9:00, she changed three dressings, reviewed two sets of discharge instructions, and had a 20-minute conversation with a 68-year-old man named Gerald Witmore, who’d had a hip replacement two days ago and wanted to talk about his tomato garden. She let him talk. He was lonely
and hurting in the specific way of someone who has spent their life being physically capable and is now confronting what it means to be dependent. And sometimes the most useful thing you can do for a person is let them talk about tomatoes. At 9:40, Marcus appeared at the end of the hallway. He was off the clock.
She could tell by the civilian clothes, jeans, and a gray sweatshirt. and he had the slightly fertive energy of someone who had come to a place they maybe shouldn’t be. He saw her and waited. She finished Gerald’s vitals, told him she’d check back at noon, and walked to the end of the hall.
“You’re not on shift,” she said. “I know.” Marcus glanced past her toward the nurse’s station. “I needed to tell you something. I’ve been thinking about it since yesterday, and if I don’t say it now, I’m going to talk myself out of it.” She waited. The transfer requests, he said, your transfer requests to the trauma unit. I work the administrative filing system on Thursdays. It’s part of my rotation.
Last month, I was pulling archived records for an insurance audit and I found your requests, all four of them. He stopped. They weren’t filed as denied. She looked at him. They were filed as not received, he said, like they never came in. But they were in the system in a subfolder in Voss’s administrative archive, not in the main personnel queue. All four of them.
The fluorescent light in the hallway hummed. Somewhere down the ward, a monitor beeped in a steady, indifferent rhythm. “You’re saying he received them and didn’t process them?” she said. “I’m saying they’re sitting in a folder that’s labeled review pending and has been since the first one came in 14 months ago.” Marcus’s jaw was tight.
I printed them. I have copies at home. I didn’t know what to do with them. And then yesterday happened and the way that Colonel talked to you and Voss going to Brenda and I just he stopped. I know this could be a problem for me. It could be, she said honestly. Depending on how you obtain the copies and what you do with them.
I obtained them in the course of an authorized audit process. I printed them because they looked anomalous and I thought they might be relevant. He met her eyes. Are they? She thought about Arthur Bellamy’s email about the phrase potential systemic suppression. About the specific way Brenda had looked away. Yes, she said they are.
Marcus nodded. He seemed both relieved and newly frightened, which was the correct response to this situation. What should I do? Don’t give them to me, she said. Not directly. If this goes where I think it might go, you want a clean chain. Contact the Federal Office of Health Systems Oversight. I’ll give you the name of the investigator.
Tell him you have documentation that may be relevant to an ongoing personnel review and ask him to advise you on proper submission protocol. Tell him Norah Callahan referred you. Do it from your personal email, not hospital accounts. She watched him absorb this. Okay, he said. and Marcus. She waited until he looked at her directly. Thank you.
I mean that. He nodded once, still frightened, and left. Norah stood in the hallway for a moment. Then she went back to Gerald Whitmore’s room and finished documenting his vitals. The call from Bellamy came at 11:17 while she was on her lunch break in the third floor break room with a cup of coffee that had gone cold.
“Malahan,” he said, “I appreciate you responding quickly. I want to be transparent with you about where the review currently stands because I think you deserve that. His voice was measured but not bureaucratic. The voice of someone who had learned to be precise without being cold. We’ve been building a case file on Callaway Regional for approximately 4 months.
Your name appeared early in the review as a personnel anomaly. someone whose record indicated a level of qualification and performance that was inconsistent with their placement and advancement history. Anomaly, she said. That’s the technical term. What I mean is that the gap between what you should have been doing there and what you were actually permitted to do is significant enough to warrant scrutiny.
What triggered the review initially? A pause. A complaint filed 8 months ago by a former Callaway Regional employee. The complaint alleged a pattern of discriminatory personnel practices targeting staff with military medical backgrounds, specifically practices that kept them from advancing into roles commensurate with their training, then use scope of practice policies to discipline them when they performed above their official capacity during crisis. She sat down the coffee.
Someone else filed this. Yes, the former employee has since taken a position at another facility. They asked to remain anonymous during the preliminary phase. She thought about who that might be. She thought about the nursing staff she’d worked alongside, the ones who’d transferred out over the past 3 years.
A name surfaced. Janet Reyes, a trauma nurse who’d left 18 months ago with a face that said she was done in ways that went beyond ordinary burnout. Janet, who had sometimes looked at Norah with an expression that balanced on the edge of saying something. She filed it and moved on. Yesterday’s event, Bellamy said, has been useful to the review.
I want to be honest, useful in ways that may accelerate things. There are witnesses. There’s documentation in the form of realtime patient records that will reflect decisions made under crisis conditions. And the presence of military personnel who can speak to your qualifications provides a form of external validation that’s significant in the context of what we’re reviewing.
You’re telling me the review is about to become an investigation. I’m telling you that a decision will likely be made within the next 72 hours about whether to escalate. And I’m calling you now because before that decision is made, I want to give you the opportunity to participate voluntarily rather than being approached formally.
What does voluntary participation look like? An interview, your own account of your experience at this facility, your personnel decisions, your employment history. It becomes part of the record in your own words before anyone else’s account of you shapes it. She looked at the cold coffee. Outside the breakroom window, the February sky was white and flat.
The kind of sky that gave nothing away. I’ll do the interview, she said. When? Tomorrow morning. If you’re available, I can come to Callaway. I’m available, she said. She hung up. The breakroom door opened and Dr. Reyes, the young doctor from yesterday, not Janet, the other Reyes, came in looking for the coffee machine.
He stopped when he saw her face, registered something in it, and then looked away with the careful neutrality of someone who had been at Callaway long enough to learn when not to ask questions. She stood, poured the cold coffee down the sink, and went back to work. The afternoon moved with the deceptive normaly of a day that is building towards something.
Norah managed her orthopedic floor patients, attended a mandatory department meeting that Brenda ran with the particular overcontrolled efficiency of someone working very hard not to look like she was managing a situation and exchanged 14 words with Voss in the hallway near the elevator. None of them significant.
All of them conducted with the surface courtesy of two people who both knew something was happening and had separately decided to wait. At 3:50, she got a text from a number she didn’t recognize. This is Sergeant Restrepo. The nurses told me your name. I wanted to say thank you for yesterday.
Both legs are still here. The doc says that mattered. She stared at it. Then she typed, “That’s the best update I’ve gotten all week. Focus on recovery. You’ve got a lot of people rooting for you.” His reply came fast. Were you really in? The guys are arguing about it. She almost smiled. Tell the guys to focus on their own recovery.
She put the phone in her pocket. The elevator opened and Brenda stepped out and for a moment they were simply standing in the corridor facing each other with nowhere else to look. Brenda had the expression of someone who had been composing a sentence for several hours and hadn’t gotten it right yet.
Nora, she said, Brenda, I want you to know. Brenda stopped, started again. I want you to know that yesterday, whatever happens administratively, yesterday was extraordinary. The outcomes, the way you managed the floor. Norah waited. I should have another stop. The composure she was known for had developed a fracture line that was becoming visible in the specific way that Brenda Pulk, who was fundamentally an honest person operating inside a dishonest structure, couldn’t quite paper over with efficiency.
There are things I should have done differently. over the past several months. “Okay,” Norah said. “I don’t expect that to fix anything.” “No,” Norah agreed. “It doesn’t.” Brenda nodded. She went to her office and closed the door. Norah rode the elevator down to the main floor, retrieved her coat from her locker, and was buttoning it when her phone rang.
James Orard. I’m calling because I think you’d want to know before it’s official, he said without preamble, which was how ord operated when something mattered. Command has submitted a formal commendation on your behalf. For yesterday’s response, it’s going into your civilian personnel record. There’s a provision for it under the veteran medical transition framework.
It’ll be public record. She leaned against the wall of the locker room. They can’t do that without my knowledge and consent, she said, not angry. Navigating. They can flag it. You have to formally accept the commendation for it to be finalized. I’m calling to ask if you will. She thought about the transfer request sitting in Voss’s subfolder for 14 months.
She thought about the four-word note. Not at this time. She thought about what it meant to have your qualifications on record somewhere that wasn’t a folder someone else controlled. Yes, she said. I’ll accept it. Good. A pause. Nora, there’s something else. She waited because with Or there was always something else.
The investigator who’s running the OSO review. Bellamy. He called my CO this afternoon. He’s broadening the inquiry. He’s looking at whether the hospital received federal certification as a veteran care facility without meeting the personnel standards that certification requires. Specifically, the standards about employing and properly utilizing staff with military medical backgrounds.
Another pause and she could hear something in it. Not hesitation, but the weight of someone delivering information that is both significant and irreversible. Nora, if that certification was obtained fraudulently or if the standards violations are severe enough, we’re not talking about individual personnel decisions anymore.
We’re talking about institutional liability at a federal level. The locker room was very quiet. Somewhere in the corridor outside, footsteps passed and faded. How many other nurses? She said, “How many others with military backgrounds at this facility?” Bellamy’s count so far is four. Three have transferred out.
You’re the only one still there. Four. She’d known there were others. She’d felt the shape of it and the way things feel when you’re inside a pattern but can’t see the whole of it. Four people. Years of accumulated suppression documented in personnel files and subfolder archives and a federal inquiry that had been building for months in the background of her ordinary days.
There’s one more thing, Ord said. and something in his voice had changed, gone quieter, and not in the controlled way of someone delivering professional information. The name of the person who filed the original complaint to OSO 8 months ago, the former employee. She had been about to say she already suspected, but she stopped because his voice was doing the thing it did when information mattered personally.
“Tell me,” she said. It was Lieutenant Colonel Diane Marsh, he said. Retired. She went by a civilian name at Callaway. You would have known her as Dolores, Norah said. The word came out before she’d finished processing what it meant. Dolores Marsh, 57, silver bracelet, three adult kids in a wallet photo, a woman who’d come into the hospital with a building pressure in her brain, and who had looked at Nora in the hallway with eyes that had, in retrospect, held something other than simple gratitude.
She was placed at Callaway 8 months ago as part of a preliminary information gathering effort, or said carefully. She took a position in hospital administration. She’s the one who submitted her initial complaint. She’s also a breath. She’s the one who forwarded Bellamy’s email to you from the anonymous administrative account.
The woman who had filed the complaint. The woman who had been in that hallway. The woman whose brain had been building toward crisis while Norah stood in the ED making calls nobody else was making. The woman Norah had caught. She stood in the locker room with the phone against her ear and the coat halfb buttoned and the sense of something enormous clicking into alignment around her.
The way things align when you finally see the whole shape of what you’ve been standing inside. Is she out of surgery? Norah said 2 hours ago. Prognosis is good. Dr. Nouku says the intervention timing was critical. Norah said I know a silence. Nora Ward said. I have to go, she said. She hung up.
She finished buttoning the coat. She stood completely still in the empty locker room for 7 seconds, which was what she allowed herself. Then she walked out and in the corridor she passed Harlon Voss coming toward her with a piece of paper in his hand and an expression that said he had made a decision and was bringing it to her in the form of official documentation.
And the paper said she could read it from 3 ft away. notice of administrative suspension pending review. And behind him, further down the corridor, she could see two people she didn’t recognize in business clothes carrying laptop bags who had the specific purposeful quality of people who know exactly where they’re going.
Voss held the paper out. She didn’t take it yet. She looked past him at the two people in business clothes who had stopped at the administrative suite and were speaking with the receptionist. and one of them turned and made brief eye contact with her just for a second, neutral and assessing and then turned back.
Voss was still holding the paper. “You’re going to want to read this,” he said. “I know what it says,” she said. “Then you know you’re suspended as of Dr. Voss.” Her voice was even level, carrying nothing that could be called emotion, which was its own form of emotion when you knew how to listen.
I think you should speak with your attorney before you hand me anything. His face changed, not dramatically. A small tightening around the eyes, a fractional shift in posture. The particular change of a person who has just understood that the ground beneath their feet is not what they thought it was. “What?” he said. Down the corridor, the two people in business clothes had been led into the administrative suite.
I think, Norah said quietly, that the next 24 hours are going to be a lot more complicated than you’re planning for. Boss’s hand was still extended when the door to the administrative suite opened again. Not the two investigators. One of them, a woman in a charcoal blazer, who moved with the brisk economy of someone whose schedule was organized down to the quarter hour.
She had a lanyard around her neck with a federal ID that caught the corridor light and she looked at Voss the way you look at a variable you’ve already accounted for. Dr. Voss, she said. Not a question. She’d known where to find him. Voss turned, his arm dropped slowly, the suspension notice still in his hand. Yes, I’m And you are? Special investigator Carla Dunore, Federal Office of Health Systems Oversight.
She held up the lanyard ID for exactly the 2 seconds required by protocol and lowered it again. We’re going to need access to the administrative personnel archive for the last 5 years, including subfolder directories. Your IT department has been notified. We’ll also need a meeting with yourself and director Hallworth at your earliest availability, which we’re defining as within the hour.
Voss looked at her. He looked at the suspension notice in his hand. He looked at Nora. Norah said nothing. She hadn’t moved. I Yes, Voss said. Of course. Can I ask what this is regarding specifically? Dunore looked at him with the particular patience of someone who has answered this question many times and has long since stopped finding it interesting.
The letter of inquiry was sent to Director Halworth’s office 6 weeks ago. It outlined the scope of the review. You can reference that document. She went back into the administrative suite. Voss stood in the corridor with the suspension notice and the look of a man trying to locate solid ground in a landscape that had just revealed itself to be mostly water.
He looked at Nora again, and this time the expression on his face was not authority. It was something smaller and more confused, the look of someone who had been so certain of the architecture of a situation that they hadn’t considered the possibility of a different floor plan. I don’t understand what’s happening, he said.
It came out more honestly than he probably intended. I know, Norah said. She meant it without cruelty. The suspension notice. I’d hold on to that for now. She walked past him and went to the elevator. Tuck. She didn’t sleep much that night. Not from anxiety exactly, more the particular restlessness that comes when something large is moving and your only available action is to wait for it. She made tea.
She didn’t finish. sat at the kitchen table with her personnel files spread in front of her and went through it the way she would have gone through any documentation before an important meeting, methodically looking for gaps, flagging things she’d need to speak to clearly. Her record at Callaway was in its way a portrait of a specific kind of institutional management.
The performance reviews were uniformly adequate, never poor, never excellent, meets expectations, reliable, good patient rapport. The language of someone being deliberately kept in the middle of the frame, never allowed to the edges where she might be seen in full. Her commendation letters from patients, there were 11, filed in a section of her record that the performance reviews never referenced, were affusive in ways the reviews weren’t. Saved my life.
The only one who actually listened. I wouldn’t be here without her. 11 letters, and not one of them cited in the documents that had determined her role for 3 years. She found the notation from her first transfer request 14 months in. Under Voss’s administrative signature, applicant does not currently meet trauma unit criteria.
Recommend reassessment in 6 months. There was no reassessment in her file. There was simply nothing. A silence where the follow-up should have been and then a second transfer request and then the same silence. Four cycles of that. Documented request, documented non-response, documented silence. She photographed each page with her phone, sent them to her personal cloud storage, and went to bed at midnight.
She lay in the dark for a while, listening to the wind move outside, and thought about Dolores Marsh in a recovery room somewhere upstairs in the hospital. She’d spent 8 months working inside while filing the paperwork that had set all of this in motion. There was something almost architectural about it, the way the pieces had moved toward each other without anyone conducting them, drawn by the logic of what had been done and what had been hidden and what was now being uncovered.
She thought about the word deliberate, whether what Voss had done was calculated strategy or simply the accumulated habit of a man who had never been required to justify his decisions about people he’d already decided didn’t matter. In her experience, those two things were harder to separate than people assumed. Indifference sustained long enough became its own form of intent.
She fell asleep at 12:40 and woke at 5:30 without an alarm. Bob Arthur Bellamy arrived at 8:15 and they met in the conference room of a law office two blocks from the hospital. Neutral ground, his suggestion, which she’d appreciated. He was a compact man in his mid-50s with reading glasses pushed up on his forehead and the unhurried manner of someone who had learned to conserve energy over long cases.
He had two assistants with laptops. There was coffee. It was better than hospital coffee, which was a low bar, but she noted it anyway. The interview lasted 3 hours and 40 minutes. She told him everything in the order he asked for it, the timeline of her transfer requests and the non-responses, the specific incidents in which her clinical recommendations had been overridden or ignored, and the patient outcomes that had followed, the performance review language and its consistent flatness, the 11 commendation letters. She
described February 11th in clinical detail, each patient, each decision, the specific gap between what the department needed and what it had. the way she’d moved into that gap because the alternative was patients dying while physicians managed their jurisdictional discomfort. She described Voss’s response, the formal report, the suspension notice.
She described Marcus without using his name yet because she told him to contact Bellamy directly and hadn’t confirmed he’d done so. Bellamy listened without interrupting. His assistants typed. When she finished, he folded his hands on the table and looked at her across the coffee cups. I want to ask you something that’s outside the formal scope of this interview, he said.
You don’t have to answer. Go ahead. At any point in 3 years, did you consider leaving? She looked at him. Yes. What kept you here? She thought about Gerald Witmore and his tomato garden. About Finn, the 9-year-old in recovery. About Dolores. The real Dolores. Before she knew who Dolores was, just a woman in a hallway with a blown pupil.
and a wallet photo and a brain that was running out of time about Curtis Albbright saying my wife in a voice that had gone thin ions, she said they were here whether I was doing it right or someone was managing me into doing it wrong. Bellamy nodded once slowly, the nod of someone who has heard many things in many rooms and knows which answers are performed and which ones aren’t.
Then he picked up his pen and they went back to the formal record. She returned to the hospital at noon. Her assignment that morning had been sent to her by text back on the orthopedic floor, same as yesterday, which meant either the administrative apparatus hadn’t processed the suspension notice or someone had quietly decided not to enforce it while investigators were walking the hallways.
She went to her locker, changed into scrubs, and was at the nurse’s station on 3x 12:15. Marcus was at the end of the hall on shift folding linen with the focused energy of someone trying to look very busy. When he saw her, he made brief eye contact and gave a small nod. He’d called Bellamy.
She could see it in the relief underneath the nerves. At 1:00, the hospitalwide intercom paged Director Warren Hallworth to the administrative suite, which was not unusual. At 120 it paged him again which was At 145 it paged him a third time and by then the nursing station on three had the low concentrated buzz of a building that knows something is happening two floors below it but can’t see exactly what.
Halworth was the hospital director. Voss’s superior, the operational head of Callaway Regional, a man Norah had met twice in three years at all staff meetings, where he’d made remarks about excellence and community partnership and the hospital’s commitment to its workforce. He had the polished aphability of someone who runs an institution by managing perception rather than operations.
And in the years she’d been watching him, she’d concluded that he was the kind of leader who was genuinely unaware of a significant portion of what happened inside his organization. not because he was negligent, but because he’d structured the layers between himself and actual operations specifically to maintain that unawareness.
The question the investigators were now working on was how much of that unawareness was deliberate. At 210, Reyes found her in the supply room. He came in under the pretense of getting something and then stood near the door and said quietly, “They pulled Voss’s email records.” She kept her face neutral. I don’t know anything about that.
I’m not saying you do. He was quiet for a moment. He was young, late 20s, she estimated, still in the phase of his career where the gap between how medicine was supposed to work and how it actually worked was visible and unsettling rather than normalized. I’ve been here 14 months. I’ve seen things I didn’t. I told myself we’re just the way it was. He stopped.
The pediatric case yesterday. If you hadn’t pushed me to call Ped’s surgery before imaging, you made the right call, she said. That’s what matters. You made me make it. Then next time you’ll make it yourself. She looked at him steadily. That’s how it’s supposed to work. He nodded.
He looked like he wanted to say something else and couldn’t find it. He left. She went back to her patients. But at 3:30, Voss was escorted out of his office. Not dramatically. This wasn’t a perp walk. No one in handcuffs. Nothing that the hallway would later reconstruct as a scene. Dunore and her colleague walked with him to the elevator, and Dunore was carrying a sealed evidence bag with what appeared to be an external hard drive inside it.
And Voss’s face had the gray compressed quality of a man experiencing something that his mental model of himself had never anticipated having to experience. Norah was at the nurse’s station on three when it happened. She didn’t see it directly. She heard about it from Darcy, who heard it from Gil, who had been in the main corridor when the elevator doors opened.
The information moved through the hospital the way information in hospitals always moves, which is to say very fast and slightly distorted by each retelling, but the core of it was consistent. Voss was gone. His access had been suspended, and Director Halworth was still in a closed meeting with the investigators and his attorney.
She processed this the way she processed most things. took it in, let it settle, didn’t let it pull her out of what she was doing. Gerald Whitmore had a follow-up appointment. A woman in bed 7 had developed a low-grade fever posh hip replacement that needed to be tracked and documented and reported. The orthopedic floor kept moving because it had to.
But there was something working underneath the ordinary progression of tasks. Something she didn’t have a precise name for. Not satisfaction exactly. Satisfaction implied a cleanness that didn’t fit. More like the feeling when weight you’ve been carrying redistributes, not disappearing, but shifting, becoming a different shape in your hands.
At 4:15, Brenda Pac called her extension. “Can you come to my office?” Brenda said. Her voice was doing the composure thing, but the composure thing had developed something unsteady under it. Norah went. Brenda’s office was small and efficiently organized in the way of someone who used order as a management strategy. She was at her desk when Norah came in and she didn’t stand and she didn’t gesture to the chair across from her desk with the practiced hospitality of their previous conversations.
She just looked at Nora with the face of a person who has been conducting an internal tribunal for approximately 36 hours and has finally reached a verdict she doesn’t like. I’ve been asked to provide the investigators with documentation of all personnel decisions I was involved in or aware of regarding staff with military backgrounds.
Brenda said, “Over the past 4 years.” Norah sat down. The chair was across from the desk and she took it, which meant this was a conversation, not a summons. “Okay,” Norah said. “I’m going to cooperate fully.” Brenda’s voice had the quality of something stated as fact because saying it out loud was the only way to make it feel true.
I should have cooperated a long time ago with different things. I want you to know that I She stopped. I was aware that your transfer requests were being held. Voss told me he was conducting a periodic review before processing them. He told me that every quarter for over a year. I accepted that. Norah looked at her. I knew it wasn’t right. Brenda said quietly.
I told myself it was his domain and he had his reasons and it wasn’t. She stopped again. It was cowardice. I want to name it that. Okay. Norah said again, not forgiving, not condemning, just receiving it because it was real and it had been said with the difficulty of something real. I also want to tell you, Brenda said that I spoke with the board chair this morning before I met with the investigators.
I told him that in my professional assessment, the events of February 11th demonstrated a level of clinical judgment and crisis management that the hospital had failed to appropriately recognize or utilize. She folded her hands on the desk. I don’t know if that matters at this point. It’s on record, Norah said. It matters. Brenda nodded.
Whatever she’d been holding in her face for the past 2 days had settled into something quieter. Not peace. Consequences don’t produce peace. They produce the particular clarifying exhaustion of someone who has stopped running from a thing. Is there anything else? Norah said. No, Brenda said. Norah went back to the floor. Mochi.
The next 72 hours moved in layers. Bellamy’s office formally escalated the Callaway regional review to a full federal investigation on the second day, which meant the scope expanded and the timelines compressed and a second team of investigators arrived from Denver on the third morning with jurisdiction that extended to financial documentation.
The hospital’s federal certification as a veteran care facility was placed under provisional suspension pending review of its personnel practices, which meant a funding freeze that the board felt immediately and which produced by the afternoon of the third day, an emergency session that ran for 4 hours.
Director Halworth resigned on the morning of the fourth day. His statement cited personal reasons, which was the diplomatic language for before the investigation’s findings are formalized, and I have more options. The board accepted the resignation without a counter offer, which was its own communication. Voss’s situation was more complex.
His email records, once extracted, contained what Bellamy’s team described in carefully neutral language as documentation of deliberate personnel management decisions that fall outside established protocol, which was the formal way of saying they’d found the emails, 17 of them over 22 months, in which he and Halworth had discussed explicitly how to manage staff with military medical backgrounds.
The language wasn’t inflammatory. It was the language of two administrators talking practically about how to maintain departmental hierarchies they defined and didn’t want disrupted. But practical and explicit in an investigation of this kind was sufficient. The board suspended Voss with cause on day four.
His hospital privileges were revoked pending the outcome of the investigation and a separate professional conduct review by the state medical board. His attorney issued a statement. Norah didn’t read it. She was on shift when she heard what from Darcy who was getting better at delivering information without editorializing which was a form of growth that Voss had left the building for the last time that afternoon.
She was in the middle of documenting a wound assessment and she finished it before she let herself think about it which was probably the right order. Marcus was offered formal witness protection status within the federal review process on day three. He’d submitted his documentation through proper channels, as she’d advised. His copies of the archive transfer requests had been authenticated against the hospital’s IT records, which confirmed the files had been accessed and deliberately misfiled.
He was also, she learned, from Bellamy’s assistant in a brief call, not the only staff member who’d come forward. Two other nurses and one physician had provided statements in the 48 hours following the initial escalation. The investigation had a momentum now that was larger than any single account. She did her shifts.
She monitored Gerald Whitmore’s recovery. She tracked Diego Restrepo’s status through the surgical notes and was glad each time she checked to see his vitals holding. She did not visit Dolores Marsh’s room because she was still processing the shape of what Dolores Marsh had done and done and been, and she needed to do that processing in her own time.
On day five, she received a formal letter from the hospital board. It was addressed to her by name, which was not how board correspondents usually arrived at nursing staff. It was signed by the board chair, a woman named Patricia Good, who had been in the role for 3 years and who Norah had seen exactly once at an all staff meeting 18 months ago. The letter was two pages.
The first page formally withdrew the suspension notice filed by Dr. Voss noted that the suspension had not been enforced and would not appear in her personnel record and offered an unambiguous statement that the events of February 11th demonstrated clinical performance at a level the hospital was committed to recognizing.
The second page contained an offer, not a transfer to the trauma unit. an interim appointment as acting director of emergency response while the board conducted a formal search for permanent hospital leadership with the explicit notation that she was among the candidates being considered for the permanent role. She read it twice.
Then she set it on the kitchen table next to her cold tea and looked at it for a while. The offer was real. She knew enough about how these things work to know it wasn’t ceremonial. The board was under enough pressure from the federal investigation that a substantive change in personnel leadership was both strategically necessary and genuinely overdue.
And her record, now that it was visible in full, made the offer logical. That was its own kind of complicated. Being recognized because the alternative had become untenable was not the same as being recognized because you were seen. She thought about what it would mean to say yes. She thought about what it would mean to say no.
She drafted a response that was neither. She went to see Dolores on the afternoon of day six. Dolores was in a private room on the fifth floor, propped up in the bed with a crossword puzzle she wasn’t doing, staring at the window. She looked smaller than she’d looked in the hallway. Not diminished exactly, just returned to the dimensions of a person who wasn’t carrying an operational mission.
The bandaging on her head was neat, the monitors quiet, and when Norah knocked on the open door and came in, Dolores put the crossword down with the expression of someone who has been waiting. “I didn’t know it would be you,” Dolores said. “In the hallway when I first came in.” Norah sat in the chair beside the bed. “I know.
I’d been in the hospital 8 months. I knew your name from the file before I knew your face.” Dolores looked at her steadily. The eyes that Norah had read as simply observant during intake were now revealing themselves as something more precise. The assessment capability of someone who had spent a career evaluating situations and people under pressure.
I’m sorry you had to catch me. I’m not. Norah said. Dolores almost smiled. No, I suppose you wouldn’t be. Why Callaway? Norah said specifically. There were 16 other hospitals in the review. because yours was the clearest case. Dolores said your record was there’s a word the investigators kept using incontrovertible.
You did everything right and it was all documented and they still managed it the way they managed it. That makes for a cleaner case. She paused also because I was angry. I spent 28 years in the army and I came out and spent 6 months watching what they do to people like us in places like this. The anger is useful, but it needs structure or it just burns through you.
So, you structured it. I structured it. Dolores looked at her window again. Outside, the February sky had finally broken. A thin line of blue at the edge of the horizon, the first real color in days. I didn’t plan on ending up in a hospital bed inside the place I was investigating. That was not in the operational plan.
How’s your head? like someone drilled a hole in it, which they did. A beat. No is good. She is. A silence between them that wasn’t uncomfortable. The monitor beeped its steady rhythm. From somewhere down the hall, a cartwheel squeaked on the lenolium in the irregular pattern that meant it needed replacing.
“The board made you an offer,” Dolores said. “It wasn’t quite a question.” Norah looked at her. “How do you know that?” because it’s the logical move and I told Bellamy 3 weeks ago it was the logical move. She turned back from the window. And because you’re sitting here instead of celebrating, which means you’re not sure? Norah said nothing.
What’s the hesitation? Dolores said, not unkindly. The voice of someone who has earned the right to ask direct questions. The hesitation, Norah said slowly, is that I spent 3 years being told what I was worth by people who had no business making that determination. And now the same institution that did that is offering to tell me what I’m worth again.
And I’m trying to figure out if the difference this time is real or if it’s just a different kind of management. Dolores was quiet for a moment. That’s a fair hesitation, she said finally. I know the difference, Dolores said, is that this time you’d be setting the terms, not waiting for them to decide what you’re allowed to do and then fighting for the margin.
You’d be in the room when the decisions get made. She looked at Nora steadily. You know what it looks like when it goes wrong. Most people who take that job don’t know that. They figure it out over years. You already know. That’s an argument for yes. It It’s an observation. The argument for yes is that there are nurses in this building right now who did what you did for 3 years and haven’t had a Dolores Marsh to build a case around them. She let that sit.
What you do with the argument is your business. Norah looked at her for a long moment. Dolores looked back, patient and direct, with the steadiness of someone who had laid down what she came to lay down, and was now simply waiting to see what grew. Norah’s phone buzzed in her pocket. She checked it.
A text from Bellamy’s office, formal in tone, asking her to call at her convenience. Standard language, but the timing wasn’t standard. She’d learned to read Bellamy’s timing. She read the message again. Something in the wording was slightly different from his usual communications. At your convenience was normal. What followed it was not.
There are additional findings from the archive review that are relevant to your file. We’d like to discuss them with you before they become part of the formal record. Additional findings. She’d given Bellamy everything she had, every request, every review, every documented incident. She thought her file was complete.
The cold, specific weight of understanding settled over her. There were things in her file she hadn’t seen. Things someone had put there were taken out of there that she hadn’t known to look for. She looked up from the phone. Dolores was watching her face. You need to go, Dolores said. I need to go, Norah said.
She stood, pocketed the phone, and was at the door when Dolores said, Callahan. She turned. Whatever’s in the file, Dolores said, you already survived it. Remember that. Norah held her gaze for a moment. Then she went. She was in the elevator going down when the doors opened on the second floor and Reyes stepped in.
He took one look at her face and went quiet, which was the right instinct. They rode down together in silence. At the ground floor, she turned toward the exit. Her phone was already in her hand. She dialed Bellamy. He answered on the first ring, which told her everything about how he’d been waiting. “Mr. Bellamy,” she said.
“What did you find?” A half-second pause. The kind that isn’t hesitation, but preparation, the breath before saying something that changes the shape of what’s already been said. “Miss Callahan,” he said, “we found a second personnel file. She stopped walking.” “A parallel file,” he continued, “maintained separately from the official hospital record.
It contains documentation going back to before your first day at Callaway Regional, before your employment application was processed. He paused. Someone built a case against you before you ever walked through the door. She stood in the lobby with the phone against her ear and people moving past her in both directions and said carefully, “Say that again.
” A parallel personnel file, Bellamy said, maintained in a separate encrypted directory on the hospital’s administrative server. Our IT forensics team found it yesterday during the archive extraction. It’s substantial. The earliest document in it is dated 11 days before your employment application was formally received. 11 days.
What’s in it? She said records pulled from a veterans affairs database. Your deployment history, your commenation record, your discharge documentation. Someone ran your name through a federal personnel system before your application was even processed and compiled what they found into a working document. A pause. The document has revision history.
It was accessed and updated at least 14 times over the course of your employment. The most recent update was 6 days before the events of February 11th. Norah walked to the wall near the main entrance and put her back to it because she needed something solid behind her while she processed this.
The lobby moved around her. visitors, staff, the ordinary traffic of a building that didn’t know what was happening in its own administrative server. Who accessed it? She said Voss’s credentials on the majority of entries. Halworth on four. And Bellamy’s pause had a quality she’d learned to identify over the past week. The pause of someone delivering the part of the information they know will land hardest.
Brenda Pulk on two. The earliest access under her credentials is 18 months ago. The second is 4 months ago, which is approximately when our review began. Norah closed her eyes for 3 seconds. Brenda sitting across the desk saying I should have done things differently, saying it was cowardice. And that was probably true and probably genuine and also insufficient because cowardice that lasts 18 months and involves actively accessing a document designed to suppress someone’s career stops being merely passive at some point and becomes
something with more weight than that word could hold. I need you to send me the file. She said I’ll have a secure copy to you within the hour. Bellamy said, “I also want to tell you, and this is outside the formal scope of my role, so take it as personal rather than professional, that what’s in this file is the kind of thing that changes the character of an investigation.
This isn’t employment mismanagement anymore. This is coordinated institutional suppression with premeditation. The state medical board is going to receive this. The VA is going to receive this. and the federal prosecutor’s office has already been briefed. The federal prosecutor’s office. She held that for a moment.
Let it settle into the correct shape. Okay. She said, “How are you doing?” Bellamy said. Another out of scope moment. And she appreciated them. They were evidence that he was still a person doing this work and not just the work itself. I’m standing up, she said. That’s the answer I’ve got right now. That’s a reasonable answer,” he said. She hung up and stood in the lobby for a moment longer.
Then she went back upstairs to finish her shift because there were still patients who needed her, and that had always been the most reliable compass she had. The secure file arrived at 6:40 that evening while she was in her car in the hospital parking lot, eating a granola bar she’d found in her coat pocket and calling it dinner.
She opened it on her phone and read it the way she read difficult things, straight through, without pausing, because pausing in the middle let the weight of each piece accumulate before you had the shape of the hole. It was worse than she’d expected and more specific than she’d feared. The document was 43 pages. It began with her service record pulled cleanly from VA databases and annotated actually annotated in Voss’s handwriting on the original scanned version with observations that ranged from clinically neutral to things that made her jaw
tighten notes like high autonomy expectation. monitor closely and deployment psych profile assertive, non-ifferential, not compatible with current unit culture. And on the page covering her combat commenation, a single underlined phrase will need to be managed carefully. Will need to be managed carefully. written before she’d set foot inside Callaway Regional, before she’d introduced herself to a single colleague or treated a single patient.
He’d known what she was before she arrived, and he’d decided before she arrived that what she was was a problem to be contained. The annotations continued through her employment, each transfer request accompanied by a note explaining why it had been held, language that was careful enough to sound administrative, but specific enough to reveal intent.
The notes referenced her deployment record not as qualification but as risk. Words like boundary issues and chain of command concerns appeared in the third month of her employment attached to an incident she remembered clearly. She had escalated a patient concern to the charge nurse over a physician’s objection had been correct and the physician had complained.
For that she had been coded as having chain of command concerns for saving a patient’s life. She had been coded as a management risk. She sat in the car for a long time after she finished reading. The parking lot was mostly empty. Late shift changeover, the building’s overnight rhythm settling in. A light snow had started, thin and unhurried, coming down in the glow of the lot’s overhead lamps.
She thought about the 11 people who had written commenation letters that no one had read. She thought about 14 months of transfer requests sitting in a subfolder. She thought about Janet Reyes, who had left 18 months ago with a face that said she was done, and about three other nurses she now knew had been managed the same way, some of them for longer than she had.
She thought about the word carefully, the specific choice of it, the assumption encoded in it, that someone with her background, her training, her record required management rather than utilization, that competence in the wrong person was a liability to be handled. She had spent 3 years inside that assumption.
She had done her work, documented everything, stayed within the lines they drew, pushed gently at the margins, and never, not once, let the accumulation of it break her open in a way that they could use. She had been right to do that, and she was furious about having had to. Both things were true.
She let them both be true, sitting in the car in the snow, because she was done managing which of her true things got to exist. Then she drove home. Papa means um the state medical board’s formal investigation of Harland Voss was announced on a Tuesday 3 weeks after February 11th. The announcement was brief and procedural, buried in the board’s weekly public digest, but Bellamy’s office had flagged it and sent it to her with a note that said simply, “First of several.
” The several proved accurate. Within 48 hours, the VA’s Office of Inspector General opened a separate inquiry into the unauthorized access of veteran personnel records for purposes unrelated to veteran care. Specifically, the use of those records to compile suppression documentation. This was the piece that Bellamy had told her would change the character of the case. And he’d been right.
Accessing veteran service records for any purpose required specific authorization and specific purpose. using them to build a preemptive case against a veteran applying for civilian employment was not an authorized purpose. It was a violation of federal statute. Voss’s attorney issued a second statement. It was longer than the first and contained the phrase context and nuance twice, which was the legal equivalent of watching a building begin to lean.
Halworth’s resignation in the context of the expanded investigation was reclassified from voluntary to consequential, a distinction that had implications for his postresignation liability. His attorney had a phone call with the federal prosecutor’s office on a Wednesday afternoon that lasted 2 hours. Norah didn’t know what was said.
She knew the outcome 2 days later when Halworth’s name appeared on a formal document as a cooperating party in the investigation, which was its own answer about how that conversation had gone. Brenda Pulk resigned on a Thursday. Her resignation letter, which became part of the administrative record and therefore accessible, was three paragraphs.
The first paragraph stated her resignation. The second acknowledged that her conduct over the period in question had fallen below the professional standard she held herself to. The third was a single sentence. I am prepared to provide full cooperation to any relevant investigative authority. It was the most honest document she’d produced in 3 years.
And Norah read it once and set it aside. The hospital board, operating now under the oversight of a federal monitor, moved quickly. They had to. The provisional funding suspension was bleeding the institution in ways that every department could feel within a week. They needed a visible credible response and visible credible responses in institutional crises require actual humans making actual decisions in actual roles.
The board chair, Patricia Good, called Norah directly on a Friday morning. I know you haven’t formally responded to the offer. Good said. She had a voice that suggested she’d run enough difficult meetings to have stopped wasting the beginning of conversations on warmth she didn’t feel. Norah appreciated the efficiency.
I’m calling to tell you that the offer has been updated. Updated how? The interim framing has been removed. We’re offering you the director of emergency response position directly with a full search waved given the circumstances. The board voted unanimously last night. A pause. We’re also prepared to formally acknowledge in writing and in your personnel file the full scope of what occurred during your employment here.
Not as a legal settlement, as a statement of institutional record. what was done to you and what should have been done differently. Norah was at her kitchen table with coffee that was actually warm for once. Outside the February cold had started its slow retreat. Still present, still sharp, but with a quality that suggested it knew it was losing.
I want to ask you something, Norah said. Go ahead. The other nurses, the three who transferred out, is the board prepared to offer them the same formal acknowledgement? a pause that was longer than Good’s usual pauses, which meant it was doing real work. That’s not something I came prepared to discuss today.
I understand, but it’s the condition. Norah kept her voice even, not aggressive, precise. What happened to me was part of a pattern. Acknowledging me without acknowledging the pattern is a press release, not an institutional record. I’m not interested in being the symbol of a problem that still has unnamed victims. Another pause.
I’ll bring it to the board. Good said. Thank you, Norah said. I’ll wait for your call. She hung up and drank her coffee. Ms. The board called back on Monday. The answer was yes. It took two more weeks to locate all three former nurses. Janet Reyes, now in Billings, a man named Thomas Okafor, who transferred to a VA hospital in Colorado, and a nurse practitioner named Sylvia Crane, who had left healthc care entirely and was working in health policy in Washington.
Bellamy’s office facilitated the contact. All three agreed to participate in the formal acknowledgement process. Sylvia Crane cried on the phone with Bellamy’s assistant, which the assistant told Nora about because she thought Nora should know, and Norah sat with that for a long time.
The formal acknowledgement document was four pages. It was signed by the board chair and countersigned by the federal monitor and entered into both the hospital’s permanent administrative record and each of the five individuals personnel files. It named what had been done, specifically without euphemism, in language that Norah had reviewed and revised twice before she was satisfied.
It named the personnel whose actions had produced those outcomes. It stated in the flat declarative language of institutional record that the five individuals in question had performed at a level of competence that had been deliberately suppressed for reasons that had nothing to do with clinical qualification. It did not use the word sorry.
Norah had removed that word in the second revision because sorry was something you said to a person, not a thing you inserted into a document, and she wasn’t interested in the document performing an emotion on the institution’s behalf. What she was interested in was the record being accurate. The record was now accurate.
She started as director of emergency response on the 1st of March. The office was small, which was fine. She’d worked in smaller spaces with higher stakes. She spent the first 3 days doing what she always did when she entered a new environment, observing, mapping, identifying the gap between how things were described and how they actually functioned.
The gap at Callaway Regional’s emergency department was predictably significant. The protocols were outdated. The triage training was inconsistent. The mass casualty response plan, the one that had been so visibly inadequate on February 11th, had last been updated four years ago and bore almost no relationship to the department’s current capacity.
She started with the triage training, not because it was the most dramatic intervention, but because it was the most necessary and the most immediate, and she’d learned over years of doing difficult work that the sequence mattered more than the scale. You didn’t fix broken systems by attacking them at their most broken point.
You fixed them by starting where the fix would hold and building out from there. She brought Reyes in as a clinical partner on the protocol updates because he was good and he knew it now and knowing it made him better. She brought Gil in on the mass casualty plan because Gil had 22 years of institutional memory that no document contained and no new hire could replicate.
She found in this work a satisfaction that was different in kind from anything she’d felt in 3 years of being managed. The specific satisfaction of a person whose capabilities have been returned to their correct function. It wasn’t clean. The department pushed back on some of the protocol changes. The way departments always push back on change with the particular friction of people whose daily habits are being asked to flex.
Two senior nurses were overtly resistant in ways she had to address directly. A physician complained that the new triage framework encroached on clinical decision-making authority. And she sat in a room with him for 40 minutes and went through the framework line by line until he understood that it didn’t encroach on anything. It just required him to be present and responsive in a way that the old framework had allowed him to avoid.
These conversations were not comfortable. She didn’t expect them to be. Comfortable conversations were rarely the ones that changed anything us. She went back to see Dolores on a Wednesday afternoon in early March when the light had finally shifted from the flat gray of winter to something with more angle and warmth in it.
Dolores was out of bed sitting in the chair by the window with actual color in her face, the crossword in her lap in a way that suggested she was actually doing it rather than using it as a prop. She looked up when Norah knocked. “You took the job,” Dolores said. “I took the job.” and Norah sat down. And it’s harder than it looked from the outside, which I knew, and more necessary than I realized, which I didn’t.
Dolores nodded with the expression of someone who has heard the specific texture of that sentence before, maybe in her own voice. The other three acknowledged. Thomas Okafor may be coming back. He’s in conversation with the board about a position in the veteran care coordination program. Janet is staying in Billings. Sylvia. Nora paused.
Sylvia said she’s not coming back to clinical work, but she said the acknowledgement mattered. She used that word mattered. Dolores looked at her window. The march light came through it at an angle that made the room feel less institutional, more like a place where a person happened to be sitting. I’ve been in this work a long time, Dolores said.
building cases, documenting patterns, sitting inside bad systems long enough to see how they hold together so you know where to apply pressure. She was quiet for a moment. I’ve seen it work. I’ve seen investigations that change nothing and ones that changed enough. The difference isn’t usually the documentation. What is it? Norah said whether there’s a person at the center of it who doesn’t break. Dolores looked at her directly.
You have to understand that you were the architecture of this case. Your file was what made it coherent. 14 months of transfer requests, 11 commenation letters, three years of performance reviews that read like someone managing a threat. Any one of those is explainable. All of them together for one person over that length of time with the parallel file sitting underneath.
That’s a pattern. Patterns are what investigators can use. She paused. But only if the person at the center of the pattern keeps showing up. I almost didn’t. Norah said, “There were days I thought about leaving.” I know. You knew it’s in your file, not Voss’s file, the real one.
Your performance reviews had a tone shift in month 19. That looks like someone who has started deciding whether the fight is worth it. Dolores said it without apology because it was information, not accusation. You stayed. I stayed because of the patience, Norah said. I want to be clear about that. It wasn’t strategy. I know that too.
Dolores said that’s what made it credible. They sat for a while in the way of two people who have said the important things and don’t need to fill the silence that comes after. Outside, a bird moved past the window. Just a brief dark shape gone before she could identify it. What’s next for you? Norah said recovery. Dolores touched the bandaging on her head with a brief pragmatic gesture.
Then there are 16 other hospitals in this review. I’ve been asked to consult on the next phase. A pause from a desk. Apparently, my field methodology needs adjustment. Norah almost laughed. It came out as something smaller but real. You got a brain surgery out of it. I got a brain surgery out of it.
Dolores agreed dryly. I’m going to put that in the methodology notes. Not recommended. Yeah. The formal state medical board hearing on Harlland Voss took place in the third week of March. Norah was not required to attend. Her documentation had been submitted. Her interview with investigators was on record, but she attended anyway because she’d earned the right to be in that room and she believed in the importance of being present for the consequences of things that had happened to you.
The hearing room was ordinary. fluorescent lights, a long table for the board, chairs for the parties and their council. Voss came in with two attorneys and the posture of a man who had convinced himself on the way in that he might still manage the outcome. She recognized that posture. She’d watched him use it throughout her employment, the forward-leaning certainty of someone who has always operated from a position of institutional power and hasn’t yet fully metabolized the information that the institution is no longer behind him. The
board chair read the findings into the record. Systematic unauthorized suppression of qualified personnel. Deliberate misuse of scope of practice policy as a disciplinary tool outside its intended function. Unauthorized compilation and use of federal veteran personnel records. A pattern of conduct across multiple staff members over a period of not less than 3 years.
Voss’s lead attorney made a statement. It contained the phrase context and nuance again and also the phrase well-intentioned administrative judgment and the board chair listened to it with an expression that did not change. The board revoked Voss’s hospital privileges permanently. His medical license was placed under a 2-year suspension with conditions for reinstatement that included a supervised practice period and ethics remediation.
The matter of the federal statute violations, the unauthorized access of VA records, was referred to the federal prosecutor’s office, where it joined the file that already contained Halworth’s cooperation agreement. Halworth had negotiated a settlement that included a significant financial penalty, a 5-year bar from administrative leadership in any federally funded medical institution, and his cooperation in the full documentation of the suppression program.
His cooperation had been, Bellamy told her, genuinely useful. He’d confirmed timelines, provided context, and explained the mechanism by which the parallel file had been kept off the standard administrative server. He’d done it, Bellamy noted, with the efficiency of a man who understood that comprehensive cooperation was his best remaining asset, which was a pragmatic rather than moral calculation.
But the outcome was the same. Norah listened to the board chair complete the findings. She watched Voss’s face process each sentence. She’d expected, she realized, to feel something large and definitive at this moment, some clean emotional payoff for 3 years of containment. What she felt instead was quieter and more complicated, something close to the feeling she’d had the first time she held a patients hand through a crisis, and they came out the other side.
Not triumph, but the specific weight of a thing that mattered, handled correctly, producing the outcome it should. Justice, she had learned, wasn’t a feeling. It was a process. And processes, when they worked, produced not catharsis, but accuracy. The world corrected to a version closer to true. That was enough. More than enough.
She drove back to Callaway Regional and went to work. W Diego Restrepo was discharged on a Thursday in late March, walking both legs as promised. She didn’t know he was leaving until Marcus appeared at her office door at 2:00 in the afternoon and said, “There’s someone at the main entrance asking for you.” She went down.
Restrepo was in civilian clothes, which made him look younger and also entirely himself, a person rather than a uniform, which was both. He had a cane he was clearly going to abandon as soon as he thought he could get away with it. Behind him, a woman who had to be his wife, same square jaw, same forwardleaning energy, was talking to a nurse and trying to hold two jackets in a hospital discharge folder at the same time.
I wanted to say it in person, Restrepo said. The text didn’t feel like enough. The text was fine, she said. No, it wasn’t. He looked at her with the directness of someone who has spent time recently thinking about the gap between what matters and what gets said. You made the call on my legs before anyone else was looking at me.
I know that my surgeon told me what that timing meant. You had a good surgical team, she said. I had you first, he said. Then I had a good surgical team. She accepted that. Not deflecting, not redirecting, just accepting it the way you accept something true that someone offers you directly. Take care of yourself, she said.
And actually do the physical therapy. all of it. Not the parts that feel redundant. He almost smiled. Yes, ma’am. She watched him walk out. Not without effort, not without the careful deliberateness of someone rebuilding what their body can do, but out. Both legs. The march light hit the glass doors and held them in it for a moment before the doors slid closed.
She stood in the lobby for a moment, then she went back upstairs. There was a staff meeting at 4:00, which she ran. It was the third she’d led since taking the role, and the difference between the first and the third was already visible in the way the room occupied itself. Fewer crossed arms, more forward posture, the particular atmospheric shift of a group that has started to believe the meetings might be for something.
She talked about the new triage framework. She talked about the mass casualty plan update, which was almost complete. She asked for feedback on two protocol changes and got it. real feedback, some of it critical, none of it hostile. And she wrote the critical feedback down because that was the point of asking.
At the end, a nurse named Petra, who had worked the orthopedic floor for 6 years and who had observed Norah’s first 3 months in the role with the careful neutrality of someone withholding judgment, raised her hand and said, “Can I ask something not about the protocols?” “Go ahead,” Norah said. “There’s a rumor that you were offered positions at two other hospitals before you took this one.
” Norah looked at her. That’s accurate. Why’d you stay? The room was quiet. Not performatively, just the natural quiet of people who actually want to hear the answer. She thought about it for a moment, not because she didn’t know, but because knowing wasn’t the same as having said it out loud. Because leaving would have been the easier thing, she said.
And the easier thing wasn’t what this place needed. She looked around the room at Reyes, who had grown 4 in. of professional spine since February. At Marcus, who had done something genuinely brave with nothing but a printed document and a willingness to be uncomfortable, at Petra, who was watching her with the careful assessment she’d always used, and which had, Norah was beginning to understand, always contained respect underneath it.
And because I’m done letting other people define which rooms I belong in, the room was quiet for a moment. Then Petra said, “Fair enough.” and picked up her copy of the triage framework and the meeting continued. She stayed late that night because directors stayed late and she was still learning the rhythms of the job and because there was something she wanted to finish.
She pulled up the formal protocol document she’d been building for 3 weeks and added the final section. mass casualty response, updated procedures, clear chain of command with specific escalation criteria that left no room for the kind of paralysis she’d walked into in February. She read it through once. It was good, not perfect. She’d already identified two places where it would need revision after the first real world test, but good, functional, grounded in how things actually worked rather than how they were supposed to work in the absence of
pressure. She saved it and emailed it to Bellamy’s office because it was now part of the documentation the federal monitor had requested on Callaway Regional’s corrective action plan. And then she emailed it to Thomas Okafor in Colorado and to Sylvia Crane in Washington because they had the same background she had and because good protocols should travel.
She shut off the office light and walked to the elevator. The hospital was in its overnight configuration, quieter, slower, the particular quality of a building holding its breath between the events that fill it. She walked through the main floor on her way out, the way she had walked it hundreds of times, past the nurses station and the waiting area and the corridor that led to the trauma bays, past the whiteboard with its patient tracking codes and dry erase marker.
She stopped at the whiteboard out of habit or something. She read the names and codes and bed numbers the way she’d read them every day for 3 years. The reflex of someone who has trained themselves to always know who is here and what they need. All of it was ordinary. Stable patients, posttop recoveries, and admission in progress.
The managed, difficult, ordinary work of keeping people alive inside a building that had decided finally to be honest about what that required. She put on her coat. She pushed through the doors into the March night, and the cold hit her, sharp and clean, carrying the specific quality of air that has decided winter is done, even if winter hasn’t agreed yet.
The parking lot was nearly empty. The sky above it was clear and full of stars. The kind of sky you forget exists when you’ve spent enough time under fluorescent lights. She stood in it for a moment, not thinking about the investigation or the protocols or the meeting or the email she still needed to send in the morning.
Just standing in the cold in the dark in the open air, the way she used to stand outside on the other side of the world when the day’s work was done and there was a moment brief real of being simply a person who was still there. She had spent three years being told in every language except the direct one that she was too much, too trained, too capable, too certain, too formed by experience that made the people around her uncomfortable.
She had spent 3 years making herself smaller than she was, not because she believed the assessment, but because the alternative was a fight that cost more than she could afford to pay in the currency of daily survival. She was done making herself smaller. Not because the world had rewarded her for being large. She knew better than that.
The world had tried persistently and with institutional apparatus to ensure that it wouldn’t. What had changed wasn’t the world’s willingness to see her. What had changed was that enough of the machinery that had been deployed to keep her invisible had been taken apart piece by piece by investigators and by her own documentation and by a woman who had lain in a hospital bed with a brain injury.
she’d sustained in the course of trying to help. And all of that machinery disassembled had revealed the shape of what it had been trying to hide, which was just her doing the work being exactly what she was. She got in her car. She drove home through the dark streets of Callaway, Montana, past the lit windows of ordinary lives, proceeding in their ordinary ways.
And she thought about the nurses she’d trained tomorrow and the protocol revision she’d make next week and the conversation she’d have with Okafor when he came in to discuss the veteran care coordination role. She thought about Dolores Marsh at a desk somewhere, annotating another file in another hospital, methodical and tireless and improbably cheerful about a process that would take years.
She thought about the 9-year-old boy named Finn who was home by now. She thought about Curtis Albbright in his garden and Patricia Albbright watching him from the window. She thought about Diego restrepo doing his physical therapy in whatever incremental stubborn way a person who has refused to lose his legs goes about reclaiming what they can do.
She thought about all the rooms she had walked into over all the years where someone had looked at her and made a calculation about what she was capable of and gotten it wrong. She thought about the specific cost of those miscalculations, the years they’d consumed, the energy she’d spent managing the distance between who she was and who she was permitted to be in those rooms.
And she thought again, not as a vow. Vows were for things you weren’t sure of, as a fact. as the simple, accurate statement of a woman who had learned the expensive way that the only rooms worth staying in were the ones where the truth of who you were was allowed to be useful. She parked in front of her house. The snow from February was gone.
The yard was still winter brown, but at the edge of it, near the fence, something was coming up through the cold ground. Small, green, improbably early, not waiting for permission. She sat in the car and looked at it for a moment. Then she went inside.
Disclaimer : This content may be created by AI for entertainment purposes. Any resemblance to real persons, events, or places is coincidental.